Lumbar Degenerative Disc Disease
Reviewed by our Healthcare Team Member

Daniel Birk, MD
Lumbar Degenerative Disc Disease: Causes, Symptoms, and Treatment Options
Lumbar degenerative disc disease (DDD) is a condition in which the intervertebral discs of the lower back gradually lose their structure, hydration, and flexibility. These discs, located between the lumbar vertebrae (L1 through L5), act as shock absorbers for the spine and allow for fluid movement of the back. When degeneration occurs, these important structures can become less effective and lead to a variety of back-related issues, including chronic pain, stiffness, and restricted mobility.
Below, we provide an overview of the causes, risk factors, common symptoms, diagnostic methods, and treatment approaches for lumbar degenerative disc disease. We also highlight our collaborative, multi-location, multi-disciplinary medical practice in the New York City metro area, where we strive to offer comprehensive spine care to patients from across New York, the United States, and around the world.
Understanding Lumbar Disc Structure
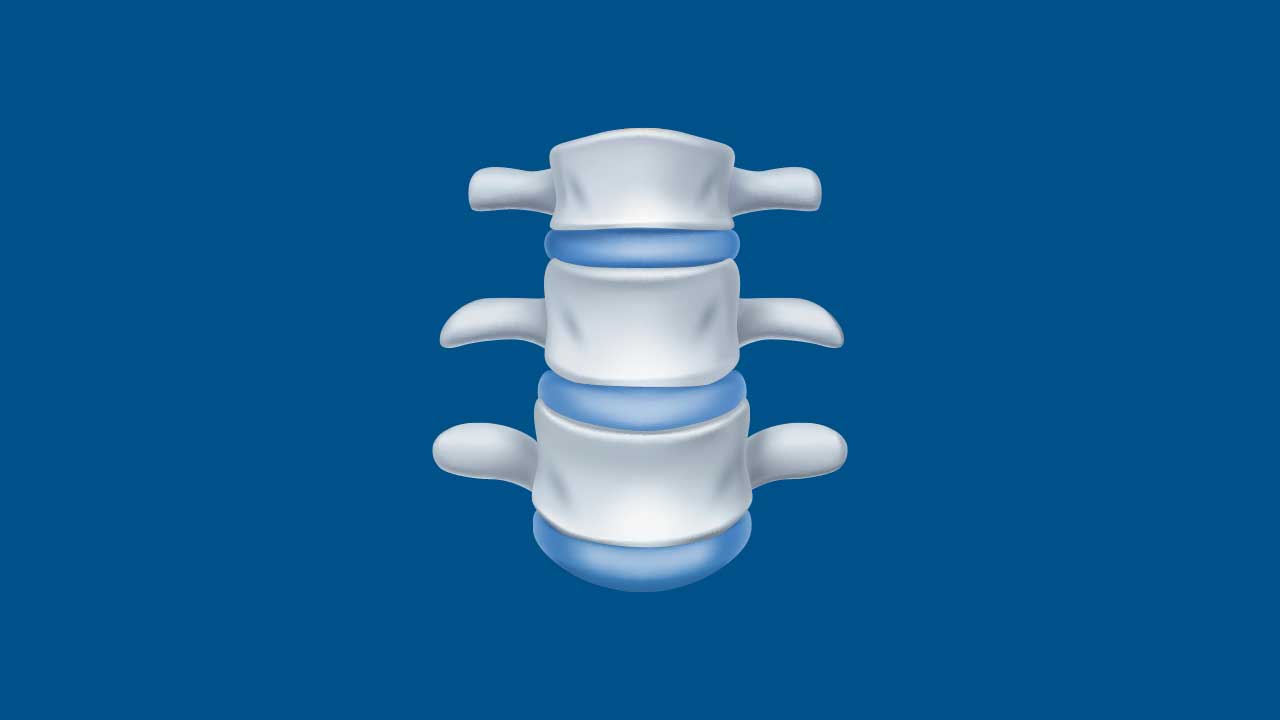
The lumbar spine consists of five vertebrae that support a significant portion of the body’s weight and facilitate a wide range of motion. Between each vertebra is an intervertebral disc, composed of two main parts:
- Nucleus Pulposus
A gel-like center that absorbs shock and helps distribute load. - Annulus Fibrosus
A tough, fibrous outer layer that keeps the nucleus pulposus contained and maintains overall disc integrity.
With degenerative disc disease, these discs can shrink, become brittle, or develop small tears over time. This process is often part of normal aging, but certain factors can accelerate or worsen disc degeneration, leading to ongoing discomfort and functional limitations.
Causes and Risk Factors
- Age-Related Wear and Tear
Over time, discs naturally lose water content, reducing their ability to cushion vertebrae and absorb shock.
Small tears in the annulus fibrosus can accumulate, leading to disc weakness. - Genetic Predisposition
A family history of spinal disorders or degenerative joint disease may increase susceptibility to disc degeneration. - Lifestyle Factors
Smoking: Nicotine reduces blood flow to the discs, hastening degeneration.
Sedentary Habits: Weak core and back muscles fail to support the spine adequately.
Obesity: Excess body weight places additional stress on the lumbar spine. - Repetitive Stress or Trauma
Certain occupations and sports involve repetitive lifting, bending, or twisting, potentially accelerating disc wear.
Acute injuries—such as from a fall or accident—can contribute to disc damage. - Underlying Conditions
Osteoarthritis: Arthritic changes in the facet joints can exacerbate stress on discs.
Scoliosis or spinal misalignment: Can unevenly distribute weight, placing added strain on certain discs.
Common Symptoms of Lumbar Degenerative Disc Disease
- Chronic Low Back Pain
A dull ache or sharp discomfort in the lower back, often worsened by prolonged sitting or standing.
Pain may fluctuate, sometimes improving with gentle movement or positional changes. - Radiating Leg Pain (Sciatica)
When disc changes cause nerve root irritation, pain may radiate down one or both legs, typically following the path of the sciatic nerve. - Stiffness and Limited Range of Motion
Difficulty bending or twisting due to pain or muscle spasms. - Weakness or Numbness
Compressed nerve roots may cause sensations of tingling, numbness, or weakness in the thighs, calves, or feet. - Pain Flare-Ups
Symptoms may worsen intermittently, often triggered by physical exertion, certain movements, or extended periods of inactivity.
Diagnosis
- Medical History and Physical Examination
Your physician will review your symptoms, daily activities, and any relevant medical background.
The exam may include tests of muscle strength, reflexes, and flexibility to identify nerve or muscle involvement. - Imaging Studies
X-ray: Can show narrowing of the disc space or bone spur formation.
MRI: Offers detailed images of the discs, nerve roots, and soft tissues, confirming the extent of degeneration.
CT Scan: May be used if MRI is not possible, often combined with myelography (contrast dye) to visualize spinal structures. - Nerve Conduction Studies / Electromyography (EMG)
Help determine if nerve compression or damage is contributing to symptoms.
Non-Surgical Treatment Options
Many individuals with lumbar degenerative disc disease find relief and improved function through conservative, non-surgical therapies, especially when diagnosed early.
- Medications
NSAIDs: Nonsteroidal anti-inflammatory drugs help manage inflammation and pain.
Muscle Relaxants: Provide short-term relief from muscle spasms.
Oral Steroids: Reduce acute inflammation around the nerve roots. - Physical Therapy
Exercise Programs: Customized exercises to strengthen the core and back muscles, improve flexibility, and alleviate spinal pressure.
Manual Therapy: Gentle manipulation and stretching to enhance spinal alignment and mobility.
Ergonomics and Posture Education: Guidance on safe body mechanics for lifting, sitting, and standing. - Spinal Injections
Epidural Steroid Injections: Steroid medication injected near the irritated nerves to decrease inflammation and temporarily ease pain.
Facet Joint Injections: If osteoarthritis or facet joint inflammation contributes to disc pain, injections may be beneficial. - Lifestyle Modification
Weight Management: Shedding extra pounds can lessen strain on spinal structures.
Smoking Cessation: Improves blood flow to discs, potentially slowing degeneration.
Low-Impact Activities: Swimming, walking, or using an elliptical trainer help maintain mobility without placing excessive stress on the spine.
Surgical Treatment Options
Surgery is considered if conservative treatments fail to provide significant relief or when advanced disc degeneration leads to persistent pain or neurological complications.
- Discectomy
Removal of herniated or damaged disc material pressing on nerve roots.
May be performed using minimally invasive methods, reducing scar tissue and recovery time. - Spinal Fusion
Fusing two or more vertebrae eliminates painful motion at the degenerated disc level.
Instruments such as rods, screws, or cages may be used to stabilize the spine while bone grafts facilitate fusion. - Artificial Disc Replacement
In select cases, replacing the damaged disc with an artificial device can preserve more spinal mobility compared to fusion. - Decompression Procedures
Laminectomy or Laminotomy: Removal or reshaping of the lamina (part of the vertebra) to create more space for nerves, which may relieve pain.
Recovery and Rehabilitation
- Postoperative Care
Depending on the procedure, hospital stays range from same-day discharge to a few days.
Pain management and mobilization strategies are tailored to each patient’s needs. - Physical Therapy
Essential for restoring strength, flexibility, and proper biomechanics following surgery or an intense flare-up.
A supervised exercise plan reduces future injury risk. - Long-Term Maintenance
Ongoing lifestyle modifications—such as regular exercise, weight management, and avoiding tobacco—are crucial to sustain improvements and prevent recurrence.
Our Multi-Disciplinary Approach in NYC
At our multi-location, multi-disciplinary medical practice in the New York City metro area, we bring together:
- Neurosurgeons and Orthopedic Spine Surgeons
- Physiatrists and Pain Management Specialists
- Physical and Occupational Therapists
- Rehabilitation Experts
This team collaborates to develop personalized treatment strategies for lumbar degenerative disc disease, leveraging advanced diagnostic tools, evidence-based therapies, and minimally invasive surgical techniques. We offer efficient coordination of care for patients throughout New York state, across the United States, and from around the world, aiming for optimal outcomes and patient satisfaction.
Additional Resources
- MedlinePlus: Degenerative Disk Disease
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIH)
Disclaimer - This article is for informational purposes only and does not replace professional medical advice. Always consult a qualified healthcare provider about any questions regarding a medical condition, diagnosis, or treatment plan.
Expert Care For This Condition Provided By

Frank Cohen, DC

Peter Roth, DC

Brian Bogdanski, DC

Alexandros Zouzias, MD

Nitin Mariwalla, MD
Daniel Birk, MD

Raymond Baule, MD

Jairus Gaberiel Flores, DPT

Samuel Brown, DO